Two new studies could change care for hundreds of thousands of heart patients.
One finds that bypass surgery has been overrated for many people with weak hearts from clogged arteries and heart attacks. The other challenges the way artery-opening procedures have been done for decades.
It was the first big test of doing balloon angioplasty to clear heart arteries through an arm instead of a leg. Complications were fewer with the arm method and at hospitals that did this more often, deaths, heart attacks and other big problems were lower, too.
The arm method is common in India, Israel, Europe and Canada, but less than five per cent of U.S. cases are done this way.
“This is the way we should be heading,” and more doctors should be trained to do it, said Dr. Edward McNulty of the University of California, San Francisco.
The bypass study’s surprising result is “a blockbuster,” McNulty said. The operation did not improve survival for heart failure patients who already were taking medicines to control risks like high cholesterol and high blood pressure.
Clogged arteries cause about two-thirds of the six million cases of heart failure in the United States. The heart isn’t getting enough blood and enlarges as it grows weaker from working too hard. Doctors often advise bypass to improve blood flow, but the new study calls that into question.
“Even if surgery is better, it’s not better by much,” said Dr. Byron Lee, a heart specialist at UCSF.
The study involved 1,200 heart failure patients in 22 countries, mostly men around 60 years old. Most had suffered a heart attack in the past. All were taking medicines they should for heart risks, and half were assigned to also get bypass surgery.
After nearly five years, about the same number in each group had died, said Dr. Eric Velazquez of Duke University Medical Center.
But its risks were evident, too. For the first two years, there were more deaths among those given surgery versus the others.
“If you don’t have an expectation to outlive that two-year window,” surgery is not a good idea, Velazquez said.
The other study involved more than 7,000 people in 32 countries getting an angiogram — a diagnostic test to look for blockages — followed by angioplasty to open any clogs found.
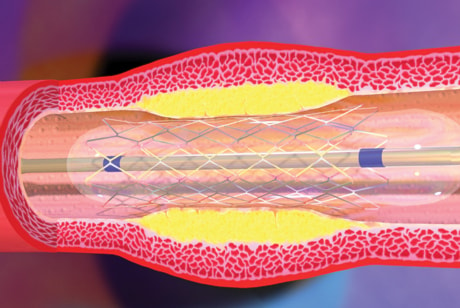
It usually involves poking a tube through a leg artery near the groin up to the heart, inflating a tiny balloon to flatten a blockage in a heart artery and placing a mesh tube called a stent to prop the artery open.
But patients can suffer major bleeding requiring transfusions or surgery, so doctors are trying this through an artery in the wrist instead.
It’s harder on doctors to do but easier on patients, who spend just a couple hours wearing a wrist band to control bleeding afterward instead of a day or more off their feet in a hospital.
The study assigned patients to get one method or the other. Survival and success rates were similar — about four per cent of each group died or had a heart attack, stroke or major bleeding in the following month.
But significantly fewer of these problems occurred in people treated with the arm method after major heart attacks, and in hospitals that did the arm method more often.
“The more you do the better you get,” and the better patients fare, said the study’s leader, Dr. Sanjit Jolly of McMaster University in Hamilton.
The study was funded by the Canadian government, a Canadian non-profit, and Sanofi-Aventis SA and Bristol-Myers Squibb Co.
(It was part of a larger study testing different doses of an anti-clotting drug used after angioplasty.)
Results were published online by the journal Lancet.
The cardiology college’s president, Dr. Ralph Brindis, said the study should be “a tipping point” to boost the arm method in the U.S.